Treponema pallidum, a name that might not be familiar to many, is the causative agent of syphilis, a disease that has been both feared and misunderstood throughout history.
This microscopic organism has a profound impact on human health, and its complex nature continues to challenge scientists and medical professionals alike.
In this blog post, we’ll look into the fascinating world of T. pallidum, exploring its categorization, transmission, pathogenesis, morphology, culture, detection, and treatment.
Categorization
Cell Wall: Gram Negative
Unlike many bacteria, T. pallidum is classified as a Gram-negative organism. Its cell wall is thin and lacks the typical structure found in Gram-positive bacteria.
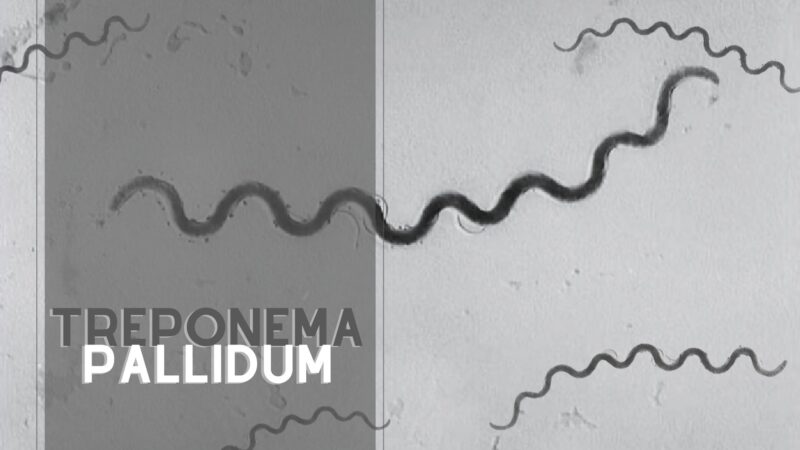
Shape: Spirochete
The spirochete shape of T. pallidum is a defining characteristic. This corkscrew-like form allows it to move in a unique way, penetrating tissues and evading the immune system.
Metabolism: Microaerophilic
T. pallidum thrives in environments with low oxygen levels, a trait known as microaerophilic metabolism. This allows it to survive in the hidden recesses of the human body.
Transmission With Sexual Contact

The vast majority of syphilitic disease is transmitted via sexual contact. However, T. pallidum can also be transmitted in utero, classifying it as part of the TORCHES Organisms, a group of pathogens that can cause congenital infections.
Pathogenesis
T. pallidum invades through exposed mucous membranes and skin, probably through micro-abrasions, and spreads throughout the body within hours after infection. This rapid dissemination makes patients contagious even before visible lesions appear.
Stages of Syphilis
The clinical consequences of syphilis follow a chronologically ordered set of events:
- Primary Syphilis: The initial stage, marked by a single sore or ulcer.
- Secondary Syphilis: Characterized by skin rashes and mucous membrane lesions.
- Latent Phase: Infection is detectable only by serological tests.
- Tertiary Syphilis: Occurs in ~30% of untreated patients, leading to severe organ damage.
Congenital Infections
Congenital syphilis possesses a different natural history and is a significant concern for pregnant women and newborns.
Morphology
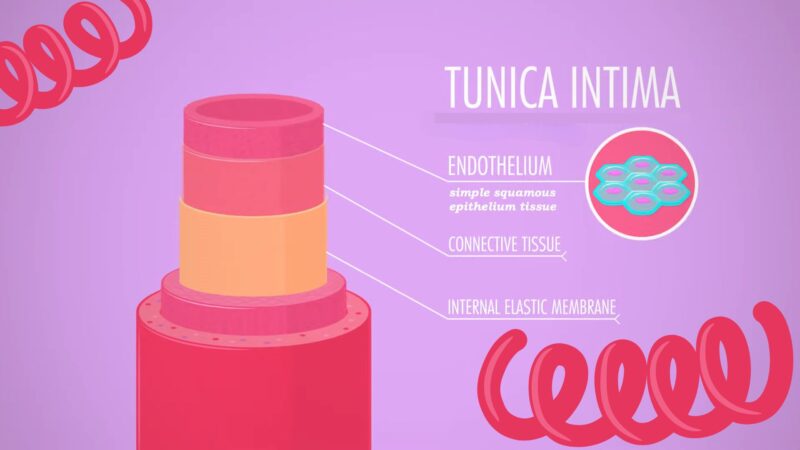
The basic morphological feature of syphilitic infection is a proliferative inflammation of the arterial tunica intima. This leads to narrowing and occlusion of blood vessels, not due to direct spirochete-mediated injury but rather the immune response to the organisms.
Culture and Detection
Microscopy and Serological Tests
Traditional light microscopy is ineffective for T. pallidum. Darkfield microscopy and immunofluorescence can detect the organisms, but serological tests are the mainstay of diagnosis.
Lab Testing
Serological tests fall into two basic categories:
- Nonspecific Treponemal Antibodies: VDRL and RPR detect antibodies to cardiolipin, used for screening and treatment monitoring.
- Specific Treponemal Antibodies: The FTA-Abs test detects antibodies specific to T. pallidum, used for confirmatory diagnosis.
Basic Approach to Diagnosis
- VDRL/RPR pos and FTA-ABS neg = False positive
- VDRL/RPR pos and FTA-ABS pos = Active infection
- VDRL/RPR neg and FTA-ABS pos = Successfully treated
- VDRL/RPR neg and FTA-ABS neg = No Syphilis, recent inoculation, or delayed immune response in AIDS Patient
Treatment
T. pallidum is highly sensitive to penicillin, making it the drug of choice. Treatment may result in a Jarisch-Herxheimer Reaction, a temporary worsening of symptoms.
FAQs
Why is There No Vaccine for Syphilis?
Developing a vaccine for syphilis has been challenging due to the complexity of T. pallidum’s outer membrane, which has too few surface proteins for an antibody to be effective. The uncertainty about the relative importance of humoral and cellular mechanisms to protective immunity has also hindered vaccine development.
How is Treponema pallidum Identified in the Laboratory?
T. pallidum can be detected with special stains like the Dieterle stain and through serology tests such as VDRL, rapid plasma reagin, and treponemal antibody tests.
What is the Significance of Treponema pallidum’s Genome Sequencing?
The genome sequencing of T. pallidum in 1998 played an essential role in understanding the bacterium’s functions, especially since it cannot be grown in pure culture. The sequencing revealed its reliance on the host for many molecules and provided insights into its adaptation to mammalian tissue.
Can Treponema pallidum be Cultivated in the Laboratory?
Long-term cultivation of T. p. pallidum in a tissue-culture system has been reported, but the bacterium cannot be grown in pure culture, making it challenging to study.
Conclusion
Treponema pallidum is a complex and elusive organism, responsible for a disease that has challenged humanity for centuries. Understanding its categorization, transmission, pathogenesis, and treatment is essential for healthcare providers and the general public alike.
With continued research and awareness, we can hope to reduce the impact of this stealthy invader on global health. Whether you’re a medical professional, a student, or simply curious about the world of microbiology, the story of T. pallidum offers a captivating glimpse into the intricate dance between pathogens and their human hosts.